Ichthyobodosis
جهت مشاهده متن کامل مقاله اینجا کلیک کنید
Ichthyobodosis (Costiosis, Ichthyobodo necator Complex)
- Ichthyobodo necator (Costia necatrix) is obligate parasite of skin and gills, and one of the smallest ectoparasites that infest fish (about the size of a red blood cell)
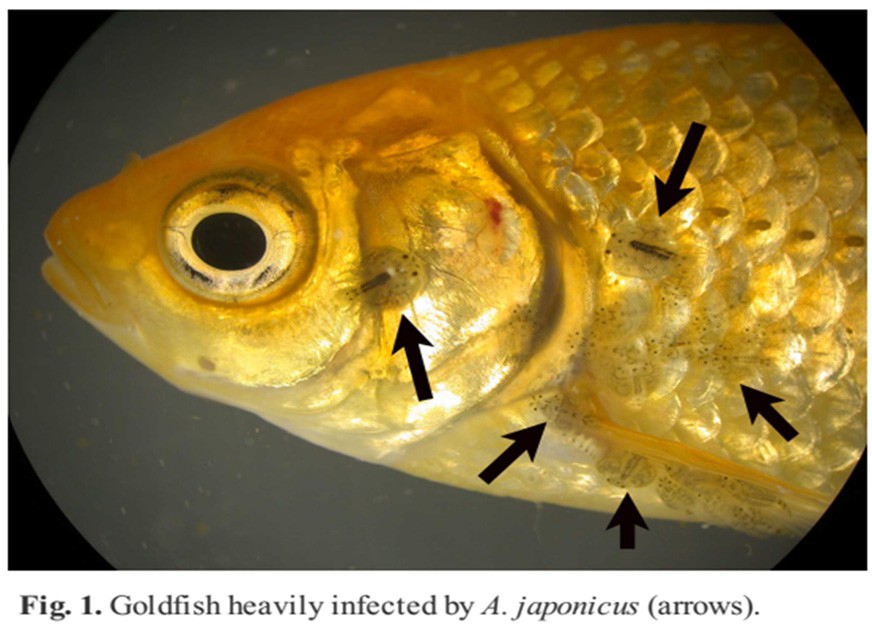
- Ichthyobodo is especially dangerous to young fish and can attack healthy fry and even eggs. In older fish it is associated with some type of predisposing stress
- Ichthyobodo necator causes disease over a wide temperature range (2– 30 °C)
- While classically a disease of freshwater fish, Ichthyobodo can survive transfer to seawater and cause mortality in marine -adapted salmonids and also occurs in purely marine fish
- Most recently, molecular genetic analysis has confirmed that this taxon is a multispecies complex (Ichthyobodo necator complex) and contains at least 9 different species with varying host preferences
Pathogenesis
Ichthyobodo exists in two forms:
The detached, mobile (free-living) form: has two or four flagella, all of which are difficult to see in actively moving parasites, measures 10–15 μm in length and is usually oval or kidney shaped
The attached form: While the parasite feeds on the fish, it is curled into a pyriform shape and is attached to and penetrates the epithelium
Clinical signs:
Ichthyobodo can cause considerable mortalities, sometimes with little obvious pathology, but other times with spongiosis and epithelial sloughing. Tissue irritation also leads to epithelial hyperplasia and increased mucus production, giving fish a bluish cast (slime)
History/Physical Examination:
typical signs include pruritus (“ flashing”), dyspnea, “ cloudy ” skin, secondary microbial infections; drop in temperature; bluish or whitish film on body
Diagnosis
- Method of Diagnosis:
- Wet mount of skin or gills with parasite
- Histopathology of skin or gills with parasite
- Diagnosis of the genus Ichthyobodo is easily made from skin or gill biopsies
- The free swimming form exhibits a characteristic flickering motion when it moves
- Attached parasites are more difficult to detect, but, in heavy infestations, they can be located by focusing up and down at high magnification on the edge of the gill epithelium, where they form palisades
- Note that cryptobids and nonpathogenic, ectocommensal bodonid flagellates may also be found on fish skin and gills; these should not be confused with Ichthyobodo
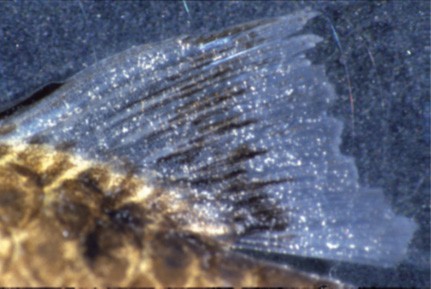
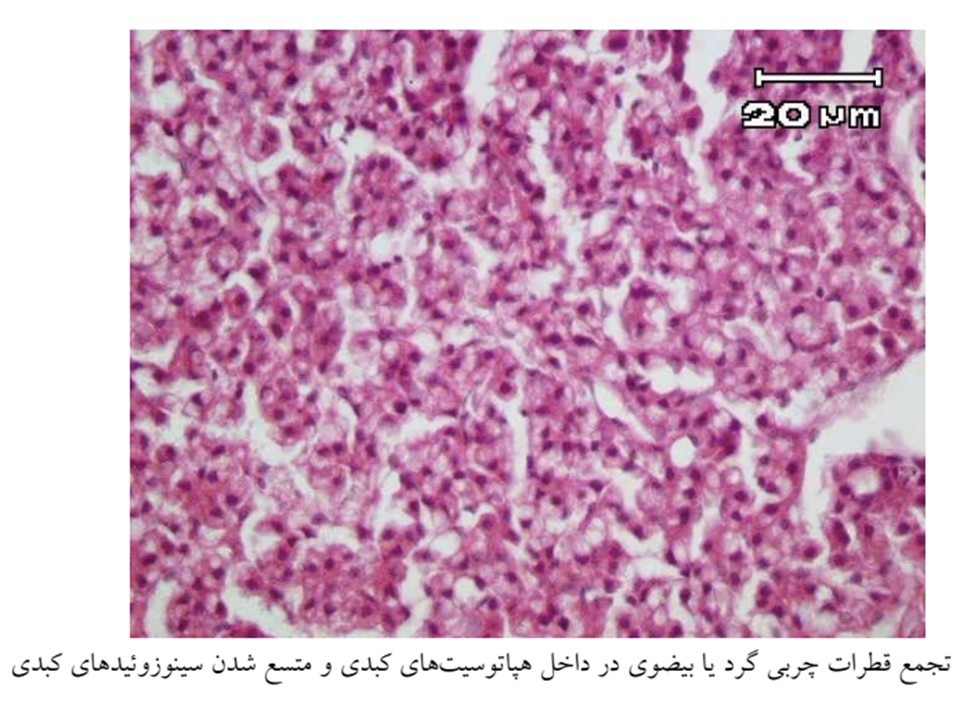
Histopathology
Histologically, there is a reduction of mucous cells early in the infection, while lamellar hyperplasia occurs in the recovery phase. Other lesions include erosive and ulcerative dermatitis
Gill lesions include exhaustion of the goblet cells, diffuse hyperplasia, sometimes with characteristic cavitation, and degeneration of epithelial and mucous cells, fusion of adjacent lamellae and cell sloughing
Damage to sub-surface cells show dramatic degeneration of the cytoplasm, although the nucleus usually remains intact
In the recovery phase, large numbers of eosinophilic granular cells may be seen within the lamellae
Treatment
Formalin bath
Formalin prolonged immersion
Potassium permanganate prolonged immersion
Raise temperature >30 °C (86° F)
Salt bath (freshwater only)
Secnidazole oral
Triclabendazole
Metronidazole oral